
COVID-19 is the name of a coronovirus disease first identified 2019-12-31, of an animal to human zoonotic event that occurred at the Huanan Seafood Wholesale Market in China. According to Wikipedia, zoonosis is an infectious disease caused by bacteria, viruses, or parasites that spread from non-human animals (usually vertebrates) to humans.
This event did not affect me personally for 56 days, until my arrival at AMS, Amsterdam Airport Schiphol, on 2020-02-25 at 9:00. It was then that I was asked if I had visited China, or had any of the known symptoms. While our flight OSL – AMS did not include anyone wearing face masks, there were at least four passengers on our AMS – SFO flight.
Since then, events have intensified.
On 2020-03-17, NRK, the Norwegian Broadcasting Corporation, was reporting that Norwegian (the airline) was refusing to transport non-Norwegian-citizen residents back to Norway. One day later, two members of my family and I did not have this problem with Delta/ KLM. Everything went smoothly. We had gone to Detroit after San Francisco. At DTW, Brock had to present his residency card in order to get a boarding card to fly from AMS to TRD. Trish and Alasdair had no problems with their Irish passports.
On arrival at TRD, a representative of the authorities boarded the plane, and read out the rules. This included 1) no tourists would be allowed to land, but would be transported back to AMS, 2) that passengers must remain quarantined for 14 days, and 3) that people with corona symptoms would not be allowed on public transport, but would have to use private vehicles. After that Norwegian citizens were allowed off the plane. Once they were off, the rest of the passengers were allowed off. That could have been about 8 people, including us. We then had to present our passports at the immigration desk. They checked our status, and allowed us in. Then we had to be inspected by the health authorities dressed in hazmat outfits. Again, we were allowed to proceed. We picked up our luggage, and ran to the train, arriving on the train platform with a minute to spare.
Alasdair used his Vy (the train company) app to buy the train tickets. There were very few people on board the train. Alasdair had to “inspect” the tickets for the conductor who, before Corona, would normally be handed the telephone and press the ticket inspection button him/her-self. We then contacted our personal food shoppers by SMS. Trish had days earlier sent them a shopping list, and now paid them using our “Vipps” (bank) app.
At Røra station, we found our car – almost without any snow on it. We then drove about 7 km to Straumen, where we picked up our groceries, from the back of the shoppers’ vehicle, and transferred them into the back of our vehicle. We talked to the shoppers who had come to the door of their house, thanking them, but keeping a distance of at least three meters. Then we drove 13 km home to Cliff Cottage.
As this is being written, there are now 6 people dead from Corona virus in Norway. The average age is 89! Our local area has opened a special emergency clinic for people with respiratory problems.
The Norwegian krone has never been so cheap (or the American dollar so expensive). Today, it was 10.50 to the dollar.
On our arrival home, we began our 14 day quarantine. Because we are symptom free, we can walk in the woods and work outside, but have to avoid people.
Covid-19 World Cup/ Superbowl
The Covid-19 World Cup/ Superbowl will be taking place on 2021-01-01. This will allow cities/ counties/ states/ countries/ regions/ continents in the world to compare themselves with all the other players. There will be winners and losers in all categories. At the very least, everyone will be comparing themselves against China.
As Oliver Milman reported: The US is on course to be severely ravaged by the coronavirus outbreak due to a delayed and dysfunctional testing regime and misleading messaging from the Trump administration, public health experts have warned. (2020-03-15 02:54) Unfortunately, this early tactic of denial will probably put USA towards the bottom of developed countries.
Milman also cited an editorial by Herbert Holden Thorp (1964 – ), a chemist, inventor and entrepreneur as well as the editor-in-chief of Science:
For the past 4 years, President Trump’s budgets have made deep cuts to science, including cuts to funding for the Centers for Disease Control and Prevention and the NIH. With this administration’s disregard for science of the Environmental Protection Agency and the National Oceanic and Atmospheric Administration, and the stalled naming of a director for the Office of Science and Technology Policy – all to support political goals – the nation has had nearly 4 years of harming and ignoring science.
Now, the president suddenly needs science. But the centuries spent elucidating fundamental principles that govern the natural world—evolution, gravity, quantum mechanics—involved laying the groundwork for knowing what we can and cannot do. The ways that scientists accumulate and analyze evidence, apply inductive reasoning, and subject findings to scrutiny by peers have been proven over the years to give rise to robust knowledge. These processes are being applied to the COVID-19 crisis through international collaboration at breakneck, unprecedented speed; Science published two new papers earlier this month on SARS-CoV-2, and more are on the way. But the same concepts that are used to describe nature are used to create new tools. So, asking for a vaccine and distorting the science at the same time are shockingly dissonant. (End quote)
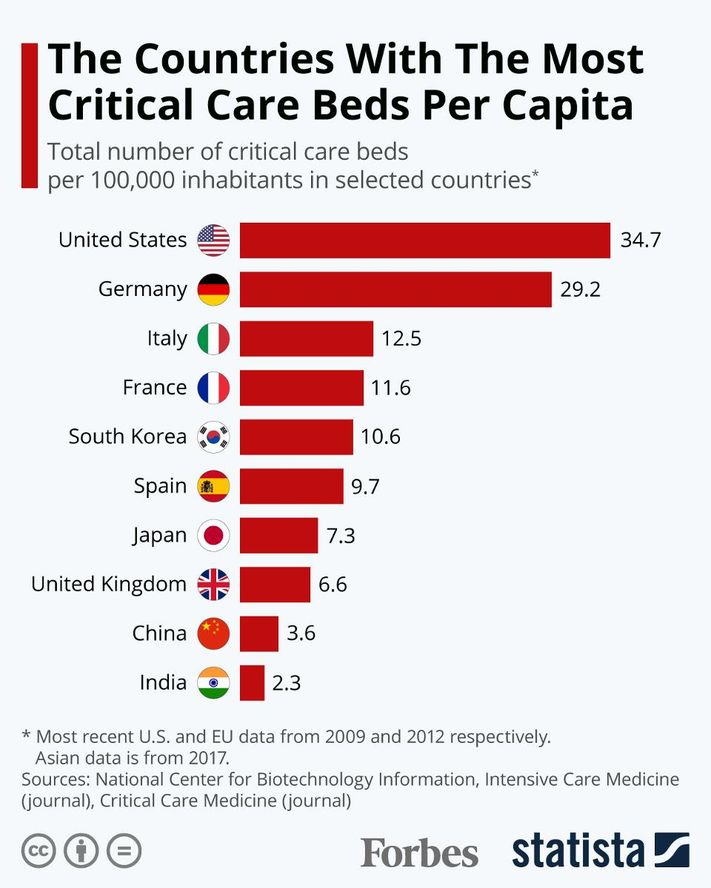
The fantastic thing about this championship is that there are any number of metrics that can be used to describe winners in contrasts to losers. Of course, politicians are not really interested in this at all. They have a vested interest in explaining why their area is fantastic, and other areas are not. Even then, not all countries/ states will be playing fairly. Some metrics can be found today. The first metric is population, along with an estimate of the percentage of people aged over 60/ 65/ 70, if this is available. Another metric available immediately, is the number of intensive care unit (ICU) beds. Figures from 2012, show this to be 8.0 per 100 000 people in Norway. More recent figures show figures for the world in the following graph.
The dates of test kit availability, and their first testing indicates how prepared the country/ state was. Indeed, the legitimacy of other metrics are, in part, dependent on the availability of these kits. At the end of the year, it will be important to know: how many people were tested; the number of positive test results, which with sufficient numbers of tests, could be an indication of the breadth of infection; the number of associated deaths. In order to compare players, data must be expressed as a percentage, or more usefully, absolute numbers per 100 000 people.
South Korea will undoubtedly emerge as the winner of the world cup/ superbowl, teaching the world how to approach similar epidemics. Given its population of 50 million, 74 new cases emerged on 2020-03-17 in contrast to 909 at its peak on 2020-02-29. Later, Reuters reported that South Korea kept new infections around a low 100 or less each day.
Numbers may yet resurge. Behind Korea’s success so far has been the most expansive and well-organized testing program in the world. This has been combined with extensive efforts to isolate infected people and trace and quarantine their contacts. South Korea has tested more than 270 000 people, (5 200 tests per million inhabitants). In contrast, USA has tested 74 per million inhabitants, according to the CDC.
“Diagnostic capacity at scale is key to epidemic control,” says Raina MacIntyre, Professor of Global Biosecurity at the University of New South Wales, Sydney. “Contact tracing is also very influential in epidemic control, as is case isolation.”
Legislation enacted in South Korea in 2015 gave the government authority to collect mobile phone, credit card, and other data from those who test positive to reconstruct their recent whereabouts. That information, stripped of personal identifiers, is shared on social media apps that allow others to determine whether they may have crossed paths with an infected person. In addition, South Korea established 43 drive-through testing stations, and in the first week of 2020-03 their Ministry of the Interior rolled out a smartphone app that can track quarantined people and collect data on symptoms.
In contrast to South Korea, and even China, USA is the developed country that I expect to come in last place. This will demonstrate that private insurance (and health care) have no place in the modern world. It may indeed indicate an end of USA’s (and capitalisms) dominance in the world, especially with respect to the economy, and innovation. In the short term, I expect a brain drain of intelligent people, and others with the opportunity to leave, from USA for places with better health care, and welfare. Canada, New Zealand and Europe will be sought after destinations. Australia and Asia, not so much. In Europe, and Italy especially, Cuba and Russia have received praise for their aid and assistance during this crisis. Perhaps these two countries will also be sought after destinations for disillusioned Americans.
In Scandinavia, there will be a regional competition between three groups of countries: Finland, Sweden and Norway/ Denmark. Finland looks as if it will be the winner.
Bjørgulv K. Bjåen writing behind a paywall in the Norwegian newspaper Vårt Land, states that Finland is in a special position. While other Nordic countries have reduced their emergency preparedness stores, the Finns have chosen to have large emergency stocks – buffers – especially with respect to drugs. In the current situation, it looks like the Finnish government will stop sales and exports of these from Finland.
Because of its Second World War experiences, Finland became a borderland between the East (The Soviet Union/ today’s Russia) and the West (Western Europe/ today’s European Union). For a decade after 1945, it had to pay major war reparations to the Soviet Union. In the process they learned to make things that they had never made before, such as icebreakers.
The contingency idea has massive support in Finland. After 1991, the Soviet Union was disbanded and four decades of a hot Cold War cooled. Sweden and Norway downsized emergency stocks, in contrast to Finland’s continued crisis thinking that embedded the principle of being prepared for surprise.
The Finnish Medicines Agency (Fimea) currently has a list of 1 400 drug types that are stored in so-called turnover stocks: One should at all times have enough for six to ten months of consumption. Manufacturers, wholesalers and hospitals rotate stock, as a matter of principle. Normal consumption is calculated from last year’s consumption.
Norway has chosen another solution. Until the EEA regulations became Norwegian law, Norway had large emergency storage facilities organized by the state medical Norwegian Medical Depot (NMD). However, after the EEA Agreement entered into force in 1994, the wholesale company changed its character; from state, to semi-state, to privatized. The Norwegian parliament (Storting) decided that the state monopoly had to be disbanded because it was in breach of EEA law. No one had told Norway to disband it.
This has resulted in the down sizing of emergency stocks, and the have been scaled down, and responsibility has spread to many players. In a report from last year, National Drug Preparedness, the Directorate of Health acknowledges major shortcomings:
“Many actors with different responsibilities for drug preparedness in Norway make the landscape unclear.”
“Only a marginal proportion of medicines consumed in Norway are produced in Norway.”
“Contingency stocks in Norway are largely concentrated in the central Eastland area, and also have inadequate content”.
“The specialist health care procurement systems are not robust in terms of drug preparedness.”
“Many municipalities have not secured emergency supplies of medicines for the health services they provide.”
“There is low awareness among the population about the importance of having a supply of necessary medicines at home.”
Sweden also recognizes that emergency storage has been replaced by the idea that most can buy something when it is needed. Last year, the Swedish Defence Research Institute analysed Sweden’s supply readiness. Finland copied Sweden’s earlier model for total defence planning and developed it further, while Sweden reduced it. There is now a shortage of drug readiness stocks.
In Sweden, emergency preparedness changed dramatically after it joined the EU in 1995.
Finland also has large emergency stocks with other important crisis products, fuels, groceries, seed, grain, metal and agricultural spare parts. Fuel stores are to secure up to five months of consumption. Grain stocks will last for six months.
In Norway, emergency grain storage facilities were closed in 2003. Today, grain storage is sufficient for only three weeks. In 2014, the Norwegian Institute for Agricultural Economics Research presented a report that said grain stocks were low.
When the right-leaning Solberg government presented the state budget for 2020, it was stated by the political parties supporting the government, that national emergency stocks for grain are not needed, because Norway can buy grain from abroad. That the supply lines are completely blocked off “for some time will not be seen as realistic”, Minister of Agriculture and Food Olaug Bollestad reported in the budget document.
Marcus Carlsson, a mathematician at Lund University, discusses two approaches to pandemics in a video, mitigation and suppression. The upper model in the video shows mitigation. This is the strategy Donald Trump appears to favour 2020-03-25, and the one implemented in Sweden. It is the same one used by South Korea, but with one major difference. To be successful, it requires extensive testing and tracking of cases, from the beginning. Until now, USA has lacked the ability to test. Yet, Trump is afraid the economy might tank without this approach. Others believe that mitigation might cost an extra million, or more, lives in USA, and take at least two years to complete. Not only that, the economy will probably still tank.
Carlsson is not an epidemiologist. He is an amateur. However, he is concerned that there is no evidence of a “herd immunity” approach controlling a virus outbreak anywhere in the world, without extensive testing. He described the Swedish government’s approach as “a mad experiment with 10 million people”.
A second approach, the lower model in Carlsson’s video, is suppression. This is the approach being used in Norway and Denmark, and in most other European countries, including two that have recently given up on the first approach – Britain and the Netherlands. According to Carlsson, this is the preferred approach, especially if there is a lack of testing. In the video he reads from a paper supporting it.
In an article in the Guardian newspaper, that describes Carlson, and comments on the 18m mark of the video, Carlson calls Sweden’s chief epidemiologist, Anders Tegnell, deceptive.
The Directorate of Health (Hdir) and the Norwegian Institute of Public Health (FHI) recommended different strategies to the government. They chose to follow Hdir and suppression, rather than FHI and mitigation. If suppression fails, then mitigation will be used.
Interestingly, Hdir has been given an overview of how much contamination equipment, including personal protective equipment (PPE), is available, but it is secret. They believe the figures will create fear, uncertainty and weaken Norway’s position in the international market if it becomes public knowledge.
FHI’s fourth risk assessment for covid-19 was published 2020-03-24. This assessment is translated into English immediately below.
In the risk assessment, FHI presents the first estimates of the number of infected in Norway with projections of the number of infected, the need for hospitalization and intensive care for the next three weeks.
- FHI recommends that the choice of strategy for the further course is postponed one to three weeks. During this period, among other things, a better basis for decision can be obtained, in particular knowledge of the effect of the measures from March 12, says Director of Public Health Institute Camilla Stoltenberg.
In the coming weeks, it is crucial to win time and fight the epidemic with measures that can significantly reduce the spread.
- A clear goal for the strategy is important. A key premise is that there is only high enough population immunity that can provide lasting protection against new, large outbreaks – this is achieved by getting many people infected or by vaccine, says Stoltenberg.
- The choice of strategy and measures is made under great uncertainty, and there is a need to obtain more and better knowledge quickly and continuously, she continues.
Prerequisites for the risk assessment
The Institute of Public Health is working to understand the situation and provide forecasts for the epidemic’s development in Norway. For this, a mathematical simulation is used together with real-world data, especially on hospital admissions.
The Institute today presents the first estimates of the number of infected persons in Norway with projections of the number of infected persons, the need for hospitalization and intensive care for the next three weeks. Thus we also have the first estimates for the dark figures in Norway.
There are still major uncertainties, and forecasts may change next week. As the epidemic progresses, FHI will have better data that can be built into the model, and the institute will adjust the model. The assumptions used in this assessment are:
- Overall mortality among infected persons below 1% (lethality).
- Severe age-related mortality; 90% of deaths in the group > 70 years.
- About 1% of all infected people will need hospitalization and ¼ of these will need mechanical breathing assistance.
- The measures should be adapted so that you get RE (the number of infections, ie how many an infected person is infected) down towards and maybe below 1.
- Depending on the strategy choice and the effect of measures, we can expect that around 5% – 50% of the population will be infected during the epidemic.
FHI’s recommended strategy
It is clear that measures to reduce the number of infections are necessary. The choice of strategy and measures is difficult and must be done under great uncertainty. There are no simple solutions, and all strategies are experiments. Decisions with potentially major ripple effects must be made under uncertainty, regardless of who takes them.
FHI recommends that the choice of strategy for the future course be postponed one to three weeks. During this period, a better basis for decision can be obtained, in particular knowledge of the effect of the measures from 12 March.
Furthermore, the institute will develop new tools to optimize testing, isolation, infection detection and quarantine. This work is in full swing and moving forward at high speed. During such a period, the burden of measures can also be analyzed, ie the negative effects of the measures on societies, businesses, groups of sick and individuals, including consequences for life and health, and build better capacity in the health service. (End of Assessment)
In Norway, we get a daily status report from FHI. A summary of this status report for 2020-03-25 follows.
A total of 2,916 infected persons have been reported. This represents 54.3 cases per 100 000 in population. Of these, 264 of the infected were reported in the last 24 hours. 00:00 to 24:00. Highlights from the day:
- 12 deaths have been notified to the Norwegian Institute of Public Health (2020-03-24 at 08.00). The average age of the dead is 84 years.
- The average age of those infected is 47.7 years, 46.8 percent are women and 53.2 percent are men.
- 1 437 people have been infected in Norway. 1 043 have been infected abroad and for 350 the infection site is being clarified. Of those infected in Norway, 724 have been close contacts of a known infected case and 671 have no known path of infection, 42 are being clarified.
- In Norway, 73 089 have been reported tested for coronavirus (SARS-CoV2) (as of 2020-03-25 at 12.00).
- 237 patients admitted to hospitals with proven covid-19 (figures from the Directorate of Health as of 2020-03-25 at 12.15). The number of admissions per day is increasing.
- There are a total of 74 persons who have been or are in intensive care with certified SARS-CoV-2, of which 51 are hospitalized (figures from the Norwegian Intensive Care Register). The average age of those admitted to intensive care is 60 years. Of these, 77% are men. (End of status report)
Politico asked 34 opinion makers how they expected COVID-19 to change the world. They comments are interesting and warrant attention. Unfortunately, Politico did not reach out to anyone at Cliff Cottage. Brock’s expectation is that this epidemic, will lead to increased ruralization. That is, the urbanization trend will be stopped, and there will be a new back to the land movement, reminiscent of the early 1970s. Activities where random people congregate will decline. These will include visits to stores, bars, cafes and restaurants, theatres and cinemas, amusement parks, casinos and sports stadiums. The concert era has ended. The cruise ship era has ended. Instead, people will focus on small-scale growing of their own crops, and entertain themselves at home, producing their own music and art.
Tim Lang, is concerned about food supply, and fragile supply chains. For several years now, I have been talking (but not doing anything practical) about the use of 15 m2 (150 square foot) geodesic domes as hydroponic greenhouses to grow foodstuffs. People without gardens can grow food on balconies. People without balconies can grow food indoors. I did buy some LED lights optimized for plant growth. However, everyone should be considering how they can grow their own supply of food.
For several years now, I have suggested purchasing an abandoned motel and setting it up as a commune. There would be a common kitchen, dining hall, and socialization area. Half of the units would be used for accommodation, half as workshops.
In terms of location, I have often wondered about – then dismissed – Ocean Falls, British Columbia. This has had an important place in my wife Patricia’s family history. Her uncle, Mort Heaps, was mill manager. Her sister, Aileen, was a nurse at the hospital. This video provides an overview of its current state.
Other locations that I have considered are located in the southern interior of British Columbia, or Vancouver Island/ Gulf Islands/ San Juan Islands/ the rain shadow of the Olympic Peninsula.
This scourge will end! For every activity that is eliminated, a new one will emerge or more likely re-emerge. There could be changes. Online shopping will predominate, while physical stores will decline. Some shopping centres may be re-purposed, but many will have to be bulldozed. Hopefully, their area (including parking lots) can be used for other purposes, including housing, recreation and urban agriculture. People will grow and process more of their own food. Hopefully, it will be healthier and more organic.