Today’s weblog post focuses on Nightscout, a social movement for Type 1 diabetics, and their parents, that enables them to access and work with continuous glucose monitor (CGM) data and open-source tools, so they are better able to manage their condition. They describe themselves as CGM in the Clouds,
In healthy people the pancreas regulates blood sugar. It works continuously without intervention. Diabetics have to take control, and inject insulin using syringes, although in recent years it has become more common to use an insulin pump connected to the body and providing an even base dose. It is difficult for people to adjust insulin levels which have to continuously monitored and adjusted for the rest of the patient’s life.
There are three main types of diabetes mellitus (DM): 1) Type 1 results from the pancreas’s failure to produce enough insulin due to a loss of beta cells; 2) Type 2 begins with insulin resistance, a condition in which cells fail to respond to insulin properly, but may result in a lack of insulin, as the disease progresses; 3) Gestational diabetes occurs when pregnant women, without a previous history of diabetes, develop high blood sugar levels.
According to the IDF Diabetes Atlas, 9th edition, an estimated 463 million people had DM worldwide (8.8% of the adult population), in 2019, with type 2 making up about 90% of the cases.
Legacy medical equipment companies, much like legacy automotive companies, perpetuate their market share by making it intolerably expensive for new companies to become established. In the automotive world, this is in part because of the extreme cost of setting up manufacturing facilities. With medical equipment, it is the cost of gaining approval in assorted jurisdictions. In the USA, for example, the Food and Drug Administration (FDA) regulates the sale of medical device products. Manufacturers (or their sales agents) must present evidence that the device is reasonably safe and effective for a particular use.
The high cost of market participation, means that legacy manufacturers can avoid/ discourage innovation, which helps improve profit margins, but denies patients access to improved technology. This is what nerds, patients and relatives have now managed to solve with Nightscout, for diabetics. It is a do-it-yourself DM tech community. It first developed data-sharing tools. More recently, an open-source closed loop artificial pancreas system has been developed.
Wikipedia says that Nightscout began in 2013-02 , when the parents of a 4-year-old boy newly diagnosed with type 1 diabetes began using a CGM system. When the child was at school there was way to access this data in real time. The boy’s father, John Costik, a software engineer, developed software to access and transfer CGM data to cloud computing infrastructure. Lane Desborough and Ross Naylor added a blood glucose chart display. A community of developers emerged to make the software generally accessible. Because this software amounted to an unlicensed medical device, it was not released immediately as open source code to address legal concerns. After this was done, the combined code was released in 2014 as the Nightscout Project.
In another part of cyberspace, Loop started off as an Apple-only framework and algorithm that runs on an iPhone, worked with older Medtronic insulin pumps and requires a small box, the RileyLink, to communicate between the pump and smartphone. It was created in large part by Pete Schwamb. An unknown number of people use this technology.
OpenAPS
The Open Artificial Pancreas System project (OpenAPS) is an open and transparent effort to make safe and effective basic artificial pancreas system technology widely available. It began in 2013, when Dana M. Lewis and Scott Leibrand became aware of the software created by John Costik. The OpenAPS software can run on a single-board computer, such as a Raspberry Pi.
Lewis, who has a DM Type 1 condition, was dissatisfied with her commercial device, because its hypoglycemic status alarm was too quiet to wake her. To address this, Lewis and Leibrand extended the CGM-in-the-cloud software to create a custom high volume alarm. They then used the same CGM-in-the-cloud software to create Do-It-Yourself Pancreas System (DIYPS) software, which provided a decision assist system for insulin delivery. This become a closed loop system using open-source decoding-carelink software created by Ben West to communicate with Medtronic insulin pumps, enabling data retrieval and issuance of insulin-dosing commands to pumps that support it. With this update, the DIYPS system became OpenAPS.
Its stated aim of OpenAPS is “to more quickly improve and save as many lives as possible and reduce the burden of Type 1 diabetes.” Their website states that “community efforts will be open source and free for use for other people, open source projects, researchers, and non-profits to use, and available on an open and non-discriminatory basis for all commercial manufacturers to use in proprietary products if desired.”
OpenAPS differs from other APS currently in clinical trials in two significant ways: 1, it is designed to use existing approved medical devices, commodity hardware, and open source software, and 2. it is designed primarily for safety, understandability, and interoperability with existing treatment approaches and existing devices. Those concerned about safety issues are encouraged to read this statement of principles.
An aside: In researching this post, one article in particular highlighted the need for professionalism in the production of code. In this case, the anonymous coder was unable to understand contextual issues. Obviously, many of the projects mentioned here have been professionally run. However, it is very common to encounter code written by amateurs, that is unsuitable for real-world use. The advantage of using people with a medical condition is that they have internalized much of the contextual information needed to produce appropriate code, even if they are amateurs.
Closed loop artificial pancreas systems integrate a glucose monitor with an insulin pump, using connecting controller software (such as assorted varieties of Loop). The system’s purpose is to keep blood glucose levels within a specified desired range for as long as possible. This can reduce damage to kidneys, retinas and nerves.
Since Nightscout is Do-It-Yourself (DIY), the onus is on the user to provide and deploy any and all resources needed, such as the MongoDB database, a web host and other software. This can result in many barriers, that prevent potential users from enjoying Nightscout’s benefits.
Recently, on 2020-11-20, Medical Data Systems LLC met with and formally petitioned the FDA for clearance of the service product “T1Pal.com.” T1Pal.com is a hosted Nightscout platform that runs copies of the latest Nightscout software on its servers for the benefit of individual subscribers.T1Pal is a hosted Nightscout platform running the latest version of Nightscout on its servers. It provides subscribers with Nightscout as a Service. This means that Medical Data Systems LLC takes responsibility for maintaining and updating the site. T1Pal was designed by Ben West, a member of the original CGM in the Cloud team and lead core developer for the Nightscout Project. A subscription costs US$ 12/ month and upwards, depending on the services provided.
Tidepool
Originally, this post had intended to focus on Tidepool, a Palo Alto, California based nonprofit company founded by Howard Look in 2013. The company works with medical equipment manufacturers, such as Dexcom and Medtronic, to create interoperable automated insulin pump systems, communicating with iPhone and Android apps.
Tidepool wanted to build a database where people with insulin-dependent diabetes could store and analyse data about their condition. Its iOS and Android apps and web system, allow users to add and view CGM related data to gain better insights into their condition. This data can be shared with health personell.
As stated in the previous weblog post on telemedicine, some equipment and software providers assume they own patient data. These companies have very disturbing privacy policies. Tidepool encouraged equipment manufacturers to develop systems that would work with Tidepool software. They elminated some of the friction, by setting up a (not-for-profit) foundation to administrate collected data.
Tidepool Loop will be its next big step, What I have been unable to discover is wny users would prefer yet another open-source closed loop artificial pancrease system, where the openAPS already seems to feature one, not to mention the RileyLook.
Developing open-source software can be messy. Sometimes, work is duplicated, and at other times, nobody is doing the work at all. The people who have a vested interest in mitigating a health condition, or in the case of Type 1 diabetes, their parents, will develop breakthrough improvements that manufacturers seldom prioritize. Software is cheap to produce, especially if development time is freely given. My expectation is that additional improvements in hardware will also come in the future, as open-hardware, as increasing numbers of people invest in CNC hardware, that can build precise equipment inexpensively.
This blogger has pre-ordered two Wyze smart watches using a facilitator in the United States, for delivery in 2020-03. This pre-order opportunity is restricted to addresses in USA, and is ending a week after the planned publication of this weblog post, on 2020-12-22. The unit price is about US$ 20, excluding taxes, shipping, non-black watch strap and who knows what else. These two watches will be used initially for experimental purposes.
The Psion Organizer II (1986) was one of the first hand-held devices, later referred to as a personal digital assistant (PDA) when Apple launched the Apple Newton (1992). Other important devices that led to today’s ubiquitous smartphone, include the Nokia 9000 Communicator (1996) and the Palm Pilot (1997) . Throughout this time frame many companies and organizations developed medical content to support the use of these devices in medical situations, including physicians’ offices and hospital wards.
Telemedicine? Telehealth? eHealth? Different people and organizations use different terms to describe the same subject. The World Health Organization (WHO) uses telemedicine to describe all aspects of remote health care including preventive care. In Europe, the more general term is eHealth, which is more than just Internet medicine, but almost everything related to computers and medicine. There is a branch of this referred to as mHealth, with a focus on hand-held devices (smartphones aka – in Europe – mobile phones = cell phones). In USA, the operative term is telehealth which also includes non-clinical services. There, telemedicine refers to remote clinical services. Here, the WHO definition is used.
The purpose of this post is to encourage people to engage in a dialogue about telemedicine, generally, but especially with the appropriate authorities where they live. They should let the world know what telemedicine services they need and want … along with additional insights and information, incorporated in the usual questions: Where?When?Why? and How?
Unfortunately, most people do not know very much about telemedicine. Thus as a first step it may be useful to read the Wikipedia article on it.
The pandemic has shown that many things need to be done differently, including health care. No prospective patients should have to travel to a (crowded?) doctor’s office to have a prescription renewed, or blood pressure measured. The first, could just involve a simple e-mail request, the second – an example of remote monitoring – could involve a patient attaching the cuff of a blood pressure monitor to their upper arm at home, in such a way that the device can measure systolic and diastolic pressure, keep track of the results in a home medical journal, and send them onwards to the appropriate health centre, especially if there is an apparent need to adjust medications or discuss lifestyle changes. In general, the advantages of telemedicine are: greater patient satisfaction and cost-effectiveness, with comparable health outcomes.
At the time of writing, Trøndelag county has the lowest incidence of COVID-19 in Europe, with less than 20 infected people per 100 000. Why? First, there are very few immigrants and other foreigners, which means that almost the entire population understands the relevant rules. There have been problems in other areas of Norway because the Norwegian government has insisted in communicating unilingually in Norwegian, and – until recently – has not made provision for translations. This means that immigrants have not been given information, in a language they understand. Second, and more importantly, people have followed the rules. They may not like them. They may complain. Yet, they follow them. Because they are followed, and the COVID-19 infection rates are reduced, there is a lighter touch in terms of regulations, than in many other areas of the world.
Update: 2020-12-08 11:34 (Less than half an hour before this is scheduled to be published). There has been a new COVID-19 outbreak in Trondheim. Maybe our county is no longer best in Europe, I don’t know. However, the outbreak seems to affect many Eritrean immigrants, and the government specifically asked them to get tested. So, even governments are learning how to do things differently.
Why is USA so different from Trøndelag? The answer may lie with Maggy Thatcher, and her good buddy, Ronny Reagan. “There is no such thing as society: there are individual men and women, and there are families,” Margaret Thatcher (1925 – 2013) said, as reported in Woman’s Own, 1987-10-31. Libertarians such as Thatcher, Ronald Reagan (1911 – 2004), Donald Trump (1946 – ), Boris Johnson (1964 – ) and more, don’t seem to believe in society, social norms, or in following rules. When people fail to follow rules in the middle of a pandemic, bad things happen.
Another problem in the US is that so much of the health care is provided by for-profit businesses, that have their own vested interests and approaches to the pandemic. They are not so much interested in reducing/ eliminating the pandemic, as they are in maximizing their profit, or at least reducing their loses. Even in Norway, there has been privitization in the health sector, that has had negative consequences.
For twenty years, or so, I had B12 injections, every three months. For the first twelve years or so, it was possible to make an appointment for an injection. Thus, I would visit the medical centre, wait perhaps five minutes, receive an injection, then leave. Then, suddenly, about the time the municipal run health service became a privately owned one, appointments for injections were no longer possible. Patients just had to take a chance and meet up. Personally, I didn’t appreciate this new system because the time spent waiting increased significantly. The health service no longer valued my time. Then, one August, I discovered that I had failed to receive an injection in May. I had met up, but the nurse was so overworked that I was asked to come back another day. Unfortunately, I quickly forgot about that, and my calendar showed a B12 shot being given. There had been no follow up from the medical centre alerting me to the missed injection. There is no reason for this lack of follow-up. It is very easy to implement in a data system. In fact, I had worked on this very type of problem earlier.
Back in the late 1980s I had worked with HUNT (Helseundersøkelse i Nord-Trøndelag. Now known in English as the Trøndelag Health Study, after the merger of Nord- and Sør-Trøndelag in 2020) and had made a mock hypertext version of their standard procedures for hypertension (high blood pressure) and diabetes. This demonstrated how data-mining of a patient journal could be used to collect data about these two conditions, and alert the patient’s doctor (and ultimately, the patient) when anomalies emerged. In 1991, one of my former students received a grant to start a company InfoTech AS, to make a real-world version of this. The major problem was that the privately-owned providers of patient journals regarded patient data as their own personal property, and would not co-operate. This was, in part, because the Norwegian government had not taken privacy concerns about patient data seriously.
Now, in 2020 in the middle of a pandemic, nobody is allowed to just meet up at a medical centre, for an injection, or anything else. Appointments have to be made for everything. When I had my annual check up with my GP, he looked at my chart, and could see immediately my one and only medication. With a new national change in policy away from B12 injections to B12 tablets, he asked me if I wanted to take B12 pills, instead of an injection? There was no doubt in my mind that I would prefer them, and so it was arranged.
What is irritating about this situation is that there should be absolutely no problem alerting everyone with a B12 deficiency problem (or any other medical situation) about tablets being allowed to substitute for injections, or any other improvement. It is simply that the medical profession is living in the past, and is not aware of the potential offered by data-mining, and similar computing techniques.
It is important for people to keep abreast of new developments, and to reflect over their own needs. They also need to contact politicians and others to make changes that will improve society. Health is important.
Ophilia (1851) by John Everett Millais (1829 – 1896).
Today (2020-05-22) is Goth Day #12. World Goth Day originated at the British Broadcasting Corporation (BBC) in 2009, when Radio 6 was looking at a number of music subcultures including Goth music. Goth DJs Cruel Britannia and Martin Oldgoth decided that May 22 would be the day each year to celebrate it.
Unfortunately, being an active Goth has a number of negative consequences. Researchers Robert Young, Helen Sweeting and Patrick West write: “identification as belonging to the Goth subculture [at some point in their lives] was the best predictor of self harm and attempted suicide [among young teens]”, and that it was most possibly due to a selection mechanism (persons that wanted to harm themselves later identified as goths, thus raising the percentage of those persons who identify as goths).”
Thus, the decision to publish this weblog post has less to do with the celebration of World Goth Day in 2020, and more to do with helping susceptible people cope with life in this challenging period of time when we all face the COVID-19 pandemic. Let us reach out with friendship and inclusion (virtually or in real-life) to those who no longer feel part of society, including those who self-identify as Goths.
In order to talk with a Goth, it might be useful to know something about Gothism!
Of course there is an official World Goth Day website complete with a list of world events. I appreciate that one of the three goths decorating this page is following COVID-19 procedures, and is equipped with a face mask.
Many attribute the start of Gothism to English author Horace Walpole (1717 – 1797) who started it off by writing The Castle of Otranto (1764). Other readers may prefer to read Ann Radcliffe’s (1764 – 1823), The Mysteries of Udolpho (1794). Washington Irving (1783 – 1859) also contributed to the genre with The Legend of Sleepy Hollow (1820), also available in its Disney animated adaption, The Adventures of Ichabod and Mr. Toad (1949). Then again there are classics such as Bram Stoker’s (1847 -1912) Dracula (1897), and Anne Rice’s (1941 – ) The Vampire Chronicles (1976).
The first mention of Gothic Rock is by music critic John Stickney to describe a meeting in a wine-cellar with Jim Morrison, described as “the perfect room to honor the Gothic rock of the Doors“. While some musicians may favour The Velvet Underground as the ultimate Gothic rock group, my own preference is for Siouxsie [Sioux aka Susan Janet Ballion (1957 – )] and the Banshees, and their track Spellbound (1981). In Norway, the Stavanger band, Theatre of Tragedy, contributed to the Gothic metal genre with its beauty and the beast aesthetic that combined harsh male with clean female vocals. Other Goth oriented bands include: Bauhaus, The Chameleons, The Cure and Sisters of Mercy.
In terms of film, the 2019 South Korean black comedy thriller, Parasite, is outstanding, and should appeal to many Goths. Another film with Gothic elements is The Rocky Horror Picture Show (1975). Because of its black humour and general lack of seriousness, it may offer a suitable dose of escapism to help people struggling to cope with a pandemic. Other relevant films in chronological order include: The Hunger (1983), Beetlejuice (1988), The Nightmare Before Christmas (1993), The Crow (1994) and The Craft (1996).
There are also computer/ console based Goth games. The Gothic role-playing game series was developed by Piranha Bytes GmbH, in Essen, Germany. It consists of three versions Gothic (2001), Gothic II (2002) and Gothic 3 (2006). There is also a fourth version, Arcania: Gothic 4 (2007), developed by Spellbound Entertainment AG, from Offenburg, Germany. This company has reorganized as Black Forest Games GmbH.
Fashionistas are undoubtedly irritated about the late reference to clothing in this weblog post. Cintra Wilson (1967 – ), writing You Just Can’t Kill It, in the New York Times 2008-09-17, notes: “The goth subculture, however, for those who live it, is more than the sum of its chicken bones, vampire clichés and existential pants. It remains a visual shortcut through which young persons of a certain damp emotional climate can broadcast to the other members of their tribe who they are. Goth is a look that simultaneously expresses and cures its own sense of alienation.”
My own approach to the Gothic was not through literature, music, film, games or fashion, but art, especially that found in the works of the Pre-Raphaelite Brotherhood. Ophelia (1851) by John Everett Millais (1829 – 1896) is one such inspiring work. In addition, John Ruskin (1819 – 1900) was particularly attracted to the Gothic in architecture, which he commented at length upon in, The Seven Lamps of Architecture (1849).
COVID-19 is the name of a coronovirus disease first identified 2019-12-31, of an animal to human zoonotic event that occurred at the Huanan Seafood Wholesale Market in China. According to Wikipedia, zoonosis is an infectious disease caused by bacteria, viruses, or parasites that spread from non-human animals (usually vertebrates) to humans.
This event did not affect me personally for 56 days, until my arrival at AMS, Amsterdam Airport Schiphol, on 2020-02-25 at 9:00. It was then that I was asked if I had visited China, or had any of the known symptoms. While our flight OSL – AMS did not include anyone wearing face masks, there were at least four passengers on our AMS – SFO flight.
Since then, events have intensified.
On 2020-03-17, NRK, the Norwegian Broadcasting Corporation, was reporting that Norwegian (the airline) was refusing to transport non-Norwegian-citizen residents back to Norway. One day later, two members of my family and I did not have this problem with Delta/ KLM. Everything went smoothly. We had gone to Detroit after San Francisco. At DTW, Brock had to present his residency card in order to get a boarding card to fly from AMS to TRD. Trish and Alasdair had no problems with their Irish passports.
On arrival at TRD, a representative of the authorities boarded the plane, and read out the rules. This included 1) no tourists would be allowed to land, but would be transported back to AMS, 2) that passengers must remain quarantined for 14 days, and 3) that people with corona symptoms would not be allowed on public transport, but would have to use private vehicles. After that Norwegian citizens were allowed off the plane. Once they were off, the rest of the passengers were allowed off. That could have been about 8 people, including us. We then had to present our passports at the immigration desk. They checked our status, and allowed us in. Then we had to be inspected by the health authorities dressed in hazmat outfits. Again, we were allowed to proceed. We picked up our luggage, and ran to the train, arriving on the train platform with a minute to spare.
Alasdair used his Vy (the train company) app to buy the train tickets. There were very few people on board the train. Alasdair had to “inspect” the tickets for the conductor who, before Corona, would normally be handed the telephone and press the ticket inspection button him/her-self. We then contacted our personal food shoppers by SMS. Trish had days earlier sent them a shopping list, and now paid them using our “Vipps” (bank) app.
At Røra station, we found our car – almost without any snow on it. We then drove about 7 km to Straumen, where we picked up our groceries, from the back of the shoppers’ vehicle, and transferred them into the back of our vehicle. We talked to the shoppers who had come to the door of their house, thanking them, but keeping a distance of at least three meters. Then we drove 13 km home to Cliff Cottage.
As this is being written, there are now 6 people dead from Corona virus in Norway. The average age is 89! Our local area has opened a special emergency clinic for people with respiratory problems.
The Norwegian krone has never been so cheap (or the American dollar so expensive). Today, it was 10.50 to the dollar.
On our arrival home, we began our 14 day quarantine. Because we are symptom free, we can walk in the woods and work outside, but have to avoid people.
Covid-19 World Cup/ Superbowl
The Covid-19 World Cup/ Superbowl will be taking place on 2021-01-01. This will allow cities/ counties/ states/ countries/ regions/ continents in the world to compare themselves with all the other players. There will be winners and losers in all categories. At the very least, everyone will be comparing themselves against China.
As Oliver Milman reported: The US is on course to be severely ravaged by the coronavirus outbreak due to a delayed and dysfunctional testing regime and misleading messaging from the Trump administration, public health experts have warned. (2020-03-15 02:54) Unfortunately, this early tactic of denial will probably put USA towards the bottom of developed countries.
Milman also cited an editorial by Herbert Holden Thorp (1964 – ), a chemist, inventor and entrepreneur as well as the editor-in-chief of Science:
For the past 4 years, President Trump’s budgets have made deep cuts to science, including cuts to funding for the Centers for Disease Control and Prevention and the NIH. With this administration’s disregard for science of the Environmental Protection Agency and the National Oceanic and Atmospheric Administration, and the stalled naming of a director for the Office of Science and Technology Policy – all to support political goals – the nation has had nearly 4 years of harming and ignoring science.
Now, the president suddenly needs science. But the centuries spent elucidating fundamental principles that govern the natural world—evolution, gravity, quantum mechanics—involved laying the groundwork for knowing what we can and cannot do. The ways that scientists accumulate and analyze evidence, apply inductive reasoning, and subject findings to scrutiny by peers have been proven over the years to give rise to robust knowledge. These processes are being applied to the COVID-19 crisis through international collaboration at breakneck, unprecedented speed; Science published two new papers earlier this month on SARS-CoV-2, and more are on the way. But the same concepts that are used to describe nature are used to create new tools. So, asking for a vaccine and distorting the science at the same time are shockingly dissonant. (End quote)
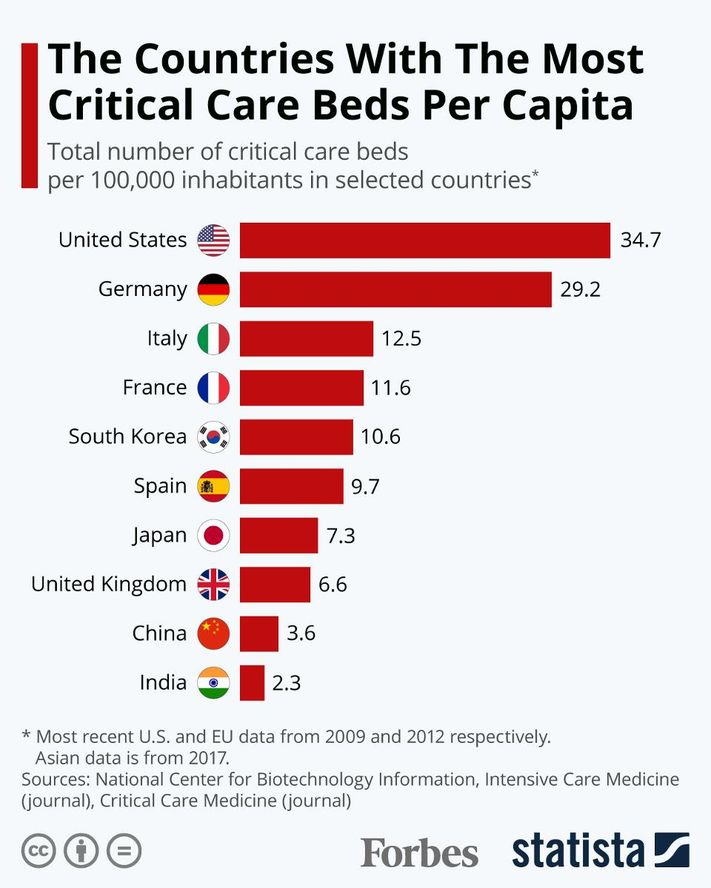
The fantastic thing about this championship is that there are any number of metrics that can be used to describe winners in contrasts to losers. Of course, politicians are not really interested in this at all. They have a vested interest in explaining why their area is fantastic, and other areas are not. Even then, not all countries/ states will be playing fairly. Some metrics can be found today. The first metric is population, along with an estimate of the percentage of people aged over 60/ 65/ 70, if this is available. Another metric available immediately, is the number of intensive care unit (ICU) beds. Figures from 2012, show this to be 8.0 per 100 000 people in Norway. More recent figures show figures for the world in the following graph.
The dates of test kit availability, and their first testing indicates how prepared the country/ state was. Indeed, the legitimacy of other metrics are, in part, dependent on the availability of these kits. At the end of the year, it will be important to know: how many people were tested; the number of positive test results, which with sufficient numbers of tests, could be an indication of the breadth of infection; the number of associated deaths. In order to compare players, data must be expressed as a percentage, or more usefully, absolute numbers per 100 000 people.
South Korea will undoubtedly emerge as the winner of the world cup/ superbowl, teaching the world how to approach similar epidemics. Given its population of 50 million, 74 new cases emerged on 2020-03-17 in contrast to 909 at its peak on 2020-02-29. Later, Reuters reported that South Korea kept new infections around a low 100 or less each day.
Numbers may yet resurge. Behind Korea’s success so far has been the most expansive and well-organized testing program in the world. This has been combined with extensive efforts to isolate infected people and trace and quarantine their contacts. South Korea has tested more than 270 000 people, (5 200 tests per million inhabitants). In contrast, USA has tested 74 per million inhabitants, according to the CDC.
“Diagnostic capacity at scale is key to epidemic control,” says Raina MacIntyre, Professor of Global Biosecurity at the University of New South Wales, Sydney. “Contact tracing is also very influential in epidemic control, as is case isolation.”
Legislation enacted in South Korea in 2015 gave the government authority to collect mobile phone, credit card, and other data from those who test positive to reconstruct their recent whereabouts. That information, stripped of personal identifiers, is shared on social media apps that allow others to determine whether they may have crossed paths with an infected person. In addition, South Korea established 43 drive-through testing stations, and in the first week of 2020-03 their Ministry of the Interior rolled out a smartphone app that can track quarantined people and collect data on symptoms.
In contrast to South Korea, and even China, USA is the developed country that I expect to come in last place. This will demonstrate that private insurance (and health care) have no place in the modern world. It may indeed indicate an end of USA’s (and capitalisms) dominance in the world, especially with respect to the economy, and innovation. In the short term, I expect a brain drain of intelligent people, and others with the opportunity to leave, from USA for places with better health care, and welfare. Canada, New Zealand and Europe will be sought after destinations. Australia and Asia, not so much. In Europe, and Italy especially, Cuba and Russia have received praise for their aid and assistance during this crisis. Perhaps these two countries will also be sought after destinations for disillusioned Americans.
In Scandinavia, there will be a regional competition between three groups of countries: Finland, Sweden and Norway/ Denmark. Finland looks as if it will be the winner.
Bjørgulv K. Bjåen writing behind a paywall in the Norwegian newspaper Vårt Land, states that Finland is in a special position. While other Nordic countries have reduced their emergency preparedness stores, the Finns have chosen to have large emergency stocks – buffers – especially with respect to drugs. In the current situation, it looks like the Finnish government will stop sales and exports of these from Finland.
Because of its Second World War experiences, Finland became a borderland between the East (The Soviet Union/ today’s Russia) and the West (Western Europe/ today’s European Union). For a decade after 1945, it had to pay major war reparations to the Soviet Union. In the process they learned to make things that they had never made before, such as icebreakers.
The contingency idea has massive support in Finland. After 1991, the Soviet Union was disbanded and four decades of a hot Cold War cooled. Sweden and Norway downsized emergency stocks, in contrast to Finland’s continued crisis thinking that embedded the principle of being prepared for surprise.
The Finnish Medicines Agency (Fimea) currently has a list of 1 400 drug types that are stored in so-called turnover stocks: One should at all times have enough for six to ten months of consumption. Manufacturers, wholesalers and hospitals rotate stock, as a matter of principle. Normal consumption is calculated from last year’s consumption.
Norway has chosen another solution. Until the EEA regulations became Norwegian law, Norway had large emergency storage facilities organized by the state medical Norwegian Medical Depot (NMD). However, after the EEA Agreement entered into force in 1994, the wholesale company changed its character; from state, to semi-state, to privatized. The Norwegian parliament (Storting) decided that the state monopoly had to be disbanded because it was in breach of EEA law. No one had told Norway to disband it.
This has resulted in the down sizing of emergency stocks, and the have been scaled down, and responsibility has spread to many players. In a report from last year, National Drug Preparedness, the Directorate of Health acknowledges major shortcomings:
“Many actors with different responsibilities for drug preparedness in Norway make the landscape unclear.”
“Only a marginal proportion of medicines consumed in Norway are produced in Norway.”
“Contingency stocks in Norway are largely concentrated in the central Eastland area, and also have inadequate content”.
“The specialist health care procurement systems are not robust in terms of drug preparedness.”
“Many municipalities have not secured emergency supplies of medicines for the health services they provide.”
“There is low awareness among the population about the importance of having a supply of necessary medicines at home.”
Sweden also recognizes that emergency storage has been replaced by the idea that most can buy something when it is needed. Last year, the Swedish Defence Research Institute analysed Sweden’s supply readiness. Finland copied Sweden’s earlier model for total defence planning and developed it further, while Sweden reduced it. There is now a shortage of drug readiness stocks.
In Sweden, emergency preparedness changed dramatically after it joined the EU in 1995.
Finland also has large emergency stocks with other important crisis products, fuels, groceries, seed, grain, metal and agricultural spare parts. Fuel stores are to secure up to five months of consumption. Grain stocks will last for six months.
In Norway, emergency grain storage facilities were closed in 2003. Today, grain storage is sufficient for only three weeks. In 2014, the Norwegian Institute for Agricultural Economics Research presented a report that said grain stocks were low.
When the right-leaning Solberg government presented the state budget for 2020, it was stated by the political parties supporting the government, that national emergency stocks for grain are not needed, because Norway can buy grain from abroad. That the supply lines are completely blocked off “for some time will not be seen as realistic”, Minister of Agriculture and Food Olaug Bollestad reported in the budget document.
Marcus Carlsson, a mathematician at Lund University, discusses two approaches to pandemics in a video, mitigation and suppression. The upper model in the video shows mitigation. This is the strategy Donald Trump appears to favour 2020-03-25, and the one implemented in Sweden. It is the same one used by South Korea, but with one major difference. To be successful, it requires extensive testing and tracking of cases, from the beginning. Until now, USA has lacked the ability to test. Yet, Trump is afraid the economy might tank without this approach. Others believe that mitigation might cost an extra million, or more, lives in USA, and take at least two years to complete. Not only that, the economy will probably still tank.
Carlsson is not an epidemiologist. He is an amateur. However, he is concerned that there is no evidence of a “herd immunity” approach controlling a virus outbreak anywhere in the world, without extensive testing. He described the Swedish government’s approach as “a mad experiment with 10 million people”.
A second approach, the lower model in Carlsson’s video, is suppression. This is the approach being used in Norway and Denmark, and in most other European countries, including two that have recently given up on the first approach – Britain and the Netherlands. According to Carlsson, this is the preferred approach, especially if there is a lack of testing. In the video he reads from a paper supporting it.
In an article in the Guardian newspaper, that describes Carlson, and comments on the 18m mark of the video, Carlson calls Sweden’s chief epidemiologist, Anders Tegnell, deceptive.
The Directorate of Health (Hdir) and the Norwegian Institute of Public Health (FHI) recommended different strategies to the government. They chose to follow Hdir and suppression, rather than FHI and mitigation. If suppression fails, then mitigation will be used.
Interestingly, Hdir has been given an overview of how much contamination equipment, including personal protective equipment (PPE), is available, but it is secret. They believe the figures will create fear, uncertainty and weaken Norway’s position in the international market if it becomes public knowledge.
FHI’s fourth risk assessment for covid-19 was published 2020-03-24. This assessment is translated into English immediately below.
In the risk assessment, FHI presents the first estimates of the number of infected in Norway with projections of the number of infected, the need for hospitalization and intensive care for the next three weeks.
FHI recommends that the choice of strategy for the further course is postponed one to three weeks. During this period, among other things, a better basis for decision can be obtained, in particular knowledge of the effect of the measures from March 12, says Director of Public Health Institute Camilla Stoltenberg.
In the coming weeks, it is crucial to win time and fight the epidemic with measures that can significantly reduce the spread.
A clear goal for the strategy is important. A key premise is that there is only high enough population immunity that can provide lasting protection against new, large outbreaks – this is achieved by getting many people infected or by vaccine, says Stoltenberg.
The choice of strategy and measures is made under great uncertainty, and there is a need to obtain more and better knowledge quickly and continuously, she continues.
Prerequisites for the risk assessment
The Institute of Public Health is working to understand the situation and provide forecasts for the epidemic’s development in Norway. For this, a mathematical simulation is used together with real-world data, especially on hospital admissions.
The Institute today presents the first estimates of the number of infected persons in Norway with projections of the number of infected persons, the need for hospitalization and intensive care for the next three weeks. Thus we also have the first estimates for the dark figures in Norway.
There are still major uncertainties, and forecasts may change next week. As the epidemic progresses, FHI will have better data that can be built into the model, and the institute will adjust the model. The assumptions used in this assessment are:
Overall mortality among infected persons below 1% (lethality).
Severe age-related mortality; 90% of deaths in the group > 70 years.
About 1% of all infected people will need hospitalization and ¼ of these will need mechanical breathing assistance.
The measures should be adapted so that you get RE (the number of infections, ie how many an infected person is infected) down towards and maybe below 1.
Depending on the strategy choice and the effect of measures, we can expect that around 5% – 50% of the population will be infected during the epidemic.
FHI’s recommended strategy
It is clear that measures to reduce the number of infections are necessary. The choice of strategy and measures is difficult and must be done under great uncertainty. There are no simple solutions, and all strategies are experiments. Decisions with potentially major ripple effects must be made under uncertainty, regardless of who takes them.
FHI recommends that the choice of strategy for the future course be postponed one to three weeks. During this period, a better basis for decision can be obtained, in particular knowledge of the effect of the measures from 12 March.
Furthermore, the institute will develop new tools to optimize testing, isolation, infection detection and quarantine. This work is in full swing and moving forward at high speed. During such a period, the burden of measures can also be analyzed, ie the negative effects of the measures on societies, businesses, groups of sick and individuals, including consequences for life and health, and build better capacity in the health service. (End of Assessment)
In Norway, we get a daily status report from FHI. A summary of this status report for 2020-03-25 follows.
A total of 2,916 infected persons have been reported. This represents 54.3 cases per 100 000 in population. Of these, 264 of the infected were reported in the last 24 hours. 00:00 to 24:00. Highlights from the day:
12 deaths have been notified to the Norwegian Institute of Public Health (2020-03-24 at 08.00). The average age of the dead is 84 years.
The average age of those infected is 47.7 years, 46.8 percent are women and 53.2 percent are men.
1 437 people have been infected in Norway. 1 043 have been infected abroad and for 350 the infection site is being clarified. Of those infected in Norway, 724 have been close contacts of a known infected case and 671 have no known path of infection, 42 are being clarified.
In Norway, 73 089 have been reported tested for coronavirus (SARS-CoV2) (as of 2020-03-25 at 12.00).
237 patients admitted to hospitals with proven covid-19 (figures from the Directorate of Health as of 2020-03-25 at 12.15). The number of admissions per day is increasing.
There are a total of 74 persons who have been or are in intensive care with certified SARS-CoV-2, of which 51 are hospitalized (figures from the Norwegian Intensive Care Register). The average age of those admitted to intensive care is 60 years. Of these, 77% are men. (End of status report)
Politico asked 34 opinion makers how they expected COVID-19 to change the world. They comments are interesting and warrant attention. Unfortunately, Politico did not reach out to anyone at Cliff Cottage. Brock’s expectation is that this epidemic, will lead to increased ruralization. That is, the urbanization trend will be stopped, and there will be a new back to the land movement, reminiscent of the early 1970s. Activities where random people congregate will decline. These will include visits to stores, bars, cafes and restaurants, theatres and cinemas, amusement parks, casinos and sports stadiums. The concert era has ended. The cruise ship era has ended. Instead, people will focus on small-scale growing of their own crops, and entertain themselves at home, producing their own music and art.
Tim Lang, is concerned about food supply, and fragile supply chains. For several years now, I have been talking (but not doing anything practical) about the use of 15 m2 (150 square foot) geodesic domes as hydroponic greenhouses to grow foodstuffs. People without gardens can grow food on balconies. People without balconies can grow food indoors. I did buy some LED lights optimized for plant growth. However, everyone should be considering how they can grow their own supply of food.
For several years now, I have suggested purchasing an abandoned motel and setting it up as a commune. There would be a common kitchen, dining hall, and socialization area. Half of the units would be used for accommodation, half as workshops.
In terms of location, I have often wondered about – then dismissed – Ocean Falls, British Columbia. This has had an important place in my wife Patricia’s family history. Her uncle, Mort Heaps, was mill manager. Her sister, Aileen, was a nurse at the hospital. This video provides an overview of its current state.
Other locations that I have considered are located in the southern interior of British Columbia, or Vancouver Island/ Gulf Islands/ San Juan Islands/ the rain shadow of the Olympic Peninsula.
This scourge will end! For every activity that is eliminated, a new one will emerge or more likely re-emerge. There could be changes. Online shopping will predominate, while physical stores will decline. Some shopping centres may be re-purposed, but many will have to be bulldozed. Hopefully, their area (including parking lots) can be used for other purposes, including housing, recreation and urban agriculture. People will grow and process more of their own food. Hopefully, it will be healthier and more organic.
On 2020-01-10 a fire broke out in a parking building at Norway’s Stavanger Airport. There were no injuries to people. However, much of the structure collapsed, including ramps to upper stories, because of structural damage caused by intense heat. Fire trucks could not enter the structure because of its low ceiling height. Because of its open walls, it was not, and was not required to be, equipped with a sprinkler system. An estimated 200 – 300 vehicles were destroyed in the fire, but about 1 300 vehicles were trapped in the building. It was initially reported the fire started in an electric vehicle. However, the fire started in a recalled diesel-powered 2005 Opel Zafira. The car was recalled after a similar fire in Cork, Ireland 2019-08-31, damaging about 60 cars in another parking structure.
Fake news, has resulted in some places in Norway banning electric cars from parking in their structures, although this is being contested by The Norwegian Electric Vehicle Association. It has sent out letters about this situation, the latest on 2020-01-21. The Norwegian Directorate for Social Security and Preparedness (DSB) states that electric cars rarely burn, but when that happens, the fire has a different course than fire in a gasoline or diesel-powered car. The fire energy is smaller and develops more slowly, but the extinguishing work must be done in a different way and may take longer.
Nils-Erik Haagenrud, Fire and Rescue Chief in Rogaland, the county where Stavanger is located, wants the county to invest in a robot that can be put into extinguishing work, when crews have to stay away from a fire, physically. Rogaland has the longest subsea tunnels in Europe, with exactly the same problems as in the parking facilities. Oslo and Romerike use robots.
Max Whirlpool (16) shown immediately after being unplugged, and waiting to be escorted outside of the kitchen, for smoking.
Max Whirlpool (16) has been expelled from the kitchen for smoking. A representative from the kitchen, who wishes to remain anonymous because he is unauthorized to speak on behalf of management, stated: “We practice tough love. There is no discrimination. Any electrical appliance caught smoking will be treated exactly the same way as Whirlpool. It will be removed from service. ” He added that Whirlpool has worked in the kitchen since 2003.
Our next microwave oven will not be a Whirlpool. That is not because of any dissatisfaction with Max, until the smoking incident. It is more related to Whirlpool as a corporation. It does not appear to take the health and safety of consumers seriously. In fact, even when one of its products was clearly to blame for a massive loss of life, 72 people, it attempted to blame others.
Recently, the Guardian reported that the Grenfell fire report “… went further than many expected, as did Moore-Bick’s dismissal of attempts by corporate groups to delay or prevent findings that might count against them, such as the “fanciful” claim by Whirlpool – the manufacturer of the Hotpoint fridge-freezer – that the fire could have been started by a cigarette.”
Earlier, the Guardian had reported on another fire, where MP Andy Slaughter said “… the government should learn from a serious fire in his constituency in 2016, when a faulty Indesit tumble dryer started a blaze in the Shepherds Court tower block in Shepherd’s Bush, west London. Residents escaped with minor injuries. Twenty fire engines and 120 firefighters attended the scene.
The same article cited a letter to UK business secretary Larry Clark, where Slaughter stated “that Whirlpool – which owns both Hotpoint and Indesit brands – had “a poor history of fire safety”.
Wikipedia, in a section titled UK Dryer Fire Risk, in its article about Whirlpool Corporation, writes: “Safety warnings about tumble dryers published on the Indesit and Hotpoint websites in 2015 advised customers that “In some rare cases, excess fluff can come into contact with the heating element and present a risk of fire.” Condensers and vented tumble dryers sold under the brands Hotpoint, Indesit, Creda, Swan and Proline and manufactured over an 11-year period between April 2004 and September 2015 present a fire risk. An estimated 5.3 million tumble dryers were bought in the UK over the time period. Originally, and even after several fires were confirmed as being caused by faulty devices, Whirlpool advised customers that using such devices was safe provided they were not left unattended but would not issue a product recall. Whirlpool offered to fix faulty machines or replace tumble dryers at a cost of £99 – an offer met with derision with consumer groups and in the press. Parliament discussed widespread difficulties with getting faulty machines fixed or replaced, including long wait times and poor service.”
Max’s replacement Sam, a Samsung MS23K3515AW purchased for NOK 900, has arrived in Inderøy. We have spent some time learning how to operate Sam. We are looking forward to working with him to serve our modest microwaving needs in the coming years: reheating food/ beverages and defrosting. Sam is originally from Malaysia.
Originally written: 2018.01.01 20:46;Updated 2019.05.03 15:00
20/20 vision is just so 19th century. In many locations it is referred to as 6/6, in Europe as 1.0. Vision acuity tests originate with their invention in 1843 by ophthalmologist Heinrich Kuechler (1811–1873), in Darmstadt, Germany.
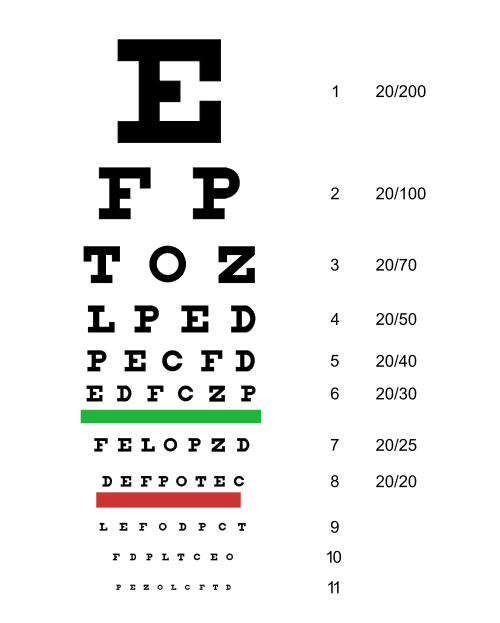
Snellen Chart (Artwork: Jeff Dahl, based on public domain document)
In 1862, Dutch ophthalmologist Herman Snellen (1834 – 1908) developed an optotype to estimate visual acuity. Optotype? Most people call it by its synonym, eye chart. In full size, the E at the top will be 88.7 mm (3.5 inches) tall. The other letters are proportionately smaller. When viewed at a distance of 20 feet = 6096 mm, normally rounded down to six meters, acuity can be estimated based on the smallest line a person can read.
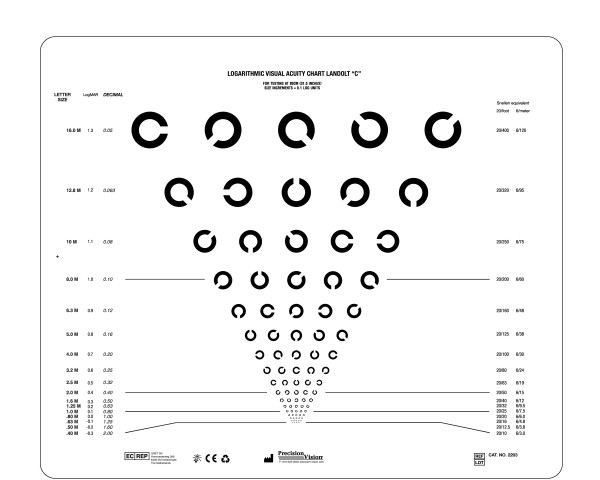
In 1888, Swiss born/ Paris resident Edmund Landolt (1846-1926) improved upon this with the Landolt C, a broken ring that uses the Snellen letter C. Both the stroke width and the gap are 1/5 of the diameter. The gap can be oriented in various positions. Normally, there are eight different alignments, each 45° apart. The person being examined must decide where the gap is. The size of the ring is reduced until a specified error rate is exceeded. The Landolt C is the standard chart used for acuity measurement in most European countries. It is specified in ISO standard 8596.
A Landolt C optotype. Not easy to find on the Internet, because many charts only show four positions, rather than the official eight.
In the first paragraph, 20/20 vision (and two equivalents) were referred to. 20/20 is just an American reference value for visual acuity. In the rest of the world this norm was called 6/6 vision. In Europe, they actually perform division on the numbers and end up with 1.0 to describe a condition where, at 6 meters distance, a human eye is able to separate contours that are approximately 1.75 mm apart. Vision of 20/40, 6/12 or 0.5 corresponds to lower, vision of 20/10, 6/3 or 2.0 to better performance.
Normal individuals have an acuity of, or better than, 20/13.3, 6/4 or 1.5, but it is dependent on age and many other factors. 20/20, 6/6 or 1.0 vision is not perfect or even particularly good acuity. It is simply good enough. To drive smaller commercial vehicles in Norway, 20/25, 6/7.5 or 0.8 acuity is required. For passenger vehicles the requirement is 20/40, 6/12 or 0.5.
This weblog post continues the story about men’s sheds. See: https://brock.mclellan.no/2019/03/03/mens-sheds/ Here, the focus is on how a shed can be used so that men can be of service to their community. As this current post is being written, a makerspace is being constructed in Inderøy, and I am looking forward to it becoming part of a world-embracing network. Locally, there are many target groups for this workshop, including that group of men who need a men’s shed. Another target group consists of pupils at Inderøy lower secondary school. Even the local Friends of the Earth group is intending to use the workshop to make controllers for a 15 square meter geodesic dome greenhouse, equipped with hydroponic gardening facilities. Full disclosure: The author is the chairperson of the Inderøy chapter of Friends of the Earth.
Purpose
People like to be of service to others, as long as they are treated fairly and with respect. At a men’s shed, it would be helpful if participants knew the type of products that people want made, using the technology that is available at the shed or makerspace. This includes, especially, products for people who have special needs, including those who feel they lack the income to keep up with changing pace of technology, or who have unique needs, not normally met with off the shelf components.
With the possession of this information secured, shedders could spend time designing low-cost products, the systems to make them, and the plans to effect their manufacture and distribution. This includes products that can enhance everyone’s enjoyment of life, as well as those that improve the life of just one single person.
While some men may have many of the necessary skill set to design, make and distribute meaningful products, others may have only some or even none of the skills. So a first step is to assess the totality of skills possessed by the men’s shed group, the specific skills each person wants to learn, and what each person wants to do with his current and future skill sets. Just because someone is an expert, or best in a group, does not mean that that person should be selected to do that specific job. Perhaps they should teach others, or learn new skills, or improve old ones.
While the current focus is to get a men’s shed up and running in Inderøy, the great thing about open source development is that development can be forked, separated into two or more branches. Locally, my interest is to ensure that people with mobility issues can have men’s sheds close to them, including in hamlets such as Mosvik (20 km from Straumen) and Beitstad (20 km from Steinkjer). In addition, I am hoping that some of these designs/ products can be of interest to men living further away, so that people can work together on them, regionally or internationally.
This requires complete documentation of each and every project, so that they can be localized. Localization is techno-speak for translating a project into the culture of a different area. For example, a project originating in the Americas, may have to have all dimensions and components metricized for use in Asia. Tools that may be legally used in USA, may be illegal in the EU and Norway, so that substitutes may have to be found. Localization becomes much more than a linguistic translation.
Struggles
At a men’s shed many different projects will be presented for the contemplation of participants. Some will be so simple, that a single person may be able to start and complete it in a matter of minutes. Others may require the efforts of many different people, over a longer period of time. When several complex projects are available, it is important that the men’s shed community, be able to prioritize, even reject. Sometimes some projects can demand skills that are not available. Sometimes they are too long, or require too many people. Regardless of the project, there must be an overview giving a reliable project timeline for people with specific skills sets, as well as other resources that are needed. In other words, one needs a project plan.
With a project plan one knows where to begin. Yet, not all projects will begin at the same place. The Open Builds project, tracks a large number of technical projects, many equipment related. When a new person or group builds a new iteration of a project, improvements can be incorporated. Again, some solutions are simple, others are incredibly complex. Fortunately, because many people throughout the world document these open source solutions, reinvention is unnecessary, Instead one can often make a generic product directly, or adapt it for a specific user.
Life can be a struggle. As trust builds in a men’s shed community, people will gradually, perhaps even reluctantly, share insights into what they are struggling with. Sometimes people need to be alone. Sometimes they need to work alone. Sometimes they need to work alone in the proximity of others. Sometimes they need to work co-operatively (but silently) with others. Sometimes they need to work co-operatively, while talking shoulder to shoulder.
This design and make process is not always easy. Many people have special needs, and insights into solving their own struggles. With a little help, they should be able to transfer those insights over to other people. Yet sometimes, indeed often, this doesn’t happen. One major reason is that mental health issues, such as anxiety or depression, divert attention.
Not all product development will deal with rocket science or cutting-edge technology. Much of it will simply involve skills with traditional equipment that shedders have used before, and feel comfortable with: Woodworking/ carpentry tools and blacksmithing/ metalworking/ welding tools. People who feel comfortable in this analog world should be encouraged to remain there, if this is what they want.
On the other hand, if they want to enter the digital world there should be a place for them there too. Much digital work at an introductory level, simply involves the copying of files, and the running of those files on a 3D printer/ CNC mill/ laser cutter, etc.
At intermediate levels, there may be a greater mismatch between the skills that are needed, and the skills that people have, so that additional training may have to be offered.
Sometimes experts will undertake the druggery necessary to bring a complex project to life. The NeuroTechnology Exploration Team lab at Rochester Institute of Technology, Henrietta, NY provides an example of how technology can be developed, then transferred throughout the world. Brain-computer interfaces (BCIs), where an individual controls computers and other devices using only their mind, is a rapidly-expanding field with a wide range of potential applications. BCI devices are especially desirable as assistive technologies for those with impaired motor or communicative capabilities. Everything the team uses in their projects is sourced and produced as cheaply as possible. The technologies used are noninvasive, relying either on electroencephalograms attached to the scalp or on localized muscle contractions, to convey signals to the computers and devices. The software is open-source and can be downloaded to any computer. For further information see: https://reporter.rit.edu/tech/brain-computer-interfacing-comes-rit
Colin Fausnaught (left), wears the Ultracortex head piece and holds the prosthetic arm, and Harrison Canning (right), wears the Ultracortex headpiece and fabric electrode sleeve at NeuroTechnology Exploration Team lab at Rochester Institute of Technology, Henrietta, N.Y. on 2019-02-01. Photo by Natalie Whitton
If open source solutions aren’t available off the shelf, a client may have to be open about his or her struggles to start the design process. This normally requires interaction, so that insights can be transferred, then developed and applied to specific problems. However that interaction does not have to be face to face. Shelagh McLellan’s bachelor degree project, On Trac (2011), was an iPad application that helped facilitate communication between teens and doctors. Teens were often able to communicate things on a tablet, that they would be too embarrassed to say directly to a doctor. For further information, see: https://cargocollective.com/shelaghjoyce/On-Trac
Many of the struggles facing people can be mitigated/ resolved through the construction of some sort of physical device (including clothing) that incorporates mechanical and electrical components, then programmed with software, to do a specific job.
An example
As stated previously, not all challenges are leading-edge. Here is an example of a widespread problem, that has multiple solutions.
I don’t like the way fruits and vegetables are sold. I dislike other people having the opportunity to handle produce/ vegetables/ fruit that I am expected to eat. I see four solutions to this problem. The first involves seeking psychological help and learning to live with the current situation. The second involves political action to ban consumers from stores and using self-driving delivery vans, packed by robots. The third involves the status quo, which means I leave the shopping to someone else. The fourth, and my preferred solution, is to grow fruit and vegetables at home. There could be many ways to do this, but I am most attracted to building a geodesic dome greenhouse, and equipping it with hydroponic gardening facilities. Personally, I would prefer to spend my time building greenhouses, and hydroponic equipment, than working in the greenhouse growing plants. My hope is to find someone to work with me on this project, someone more interested in growing and tending plants, perhaps the same person who currently does my shopping. This is the same solution that is being explored by the local Friends of the Earth chapter in Inderøy.
Poverty
One issue that cannot be ignored is that of poverty. Many of the challenges people face are caused by being unable to afford the products that will solve their problems. There are different degrees of poverty. Extreme poverty can result in emaciation and homelessness; more moderate poverty results in obesity and sub-standard living conditions. People put on weight, because the food they need is just too expensive. Thus, they feel they don’t have the economic freedom or economic opportunities that they would like. Some younger people feel that they don’t have the opportunity to purchase a house, and will end up being life-long renters, or worse. Some older people feel that they do not have the resources to buy even necessities, such as heat, because energy cost too much.
Insight
I don’t want to know anything about a client/ readers’ personal situation. That is a private matter. If someone wants a men’s shed to help with a struggle please wait until a men’s shed is established, or (help) start one yourself.
Here is the information I think a men’s shed would need to know in order to work on an extensive project for a potential client. A simple one or two day project involving a few people making something simple, does not need this level of detail.
Please describe the client in general terms: Approximate age and gender; living environment – urban or rural, living alone or with others (yes, dogs are included in the others category); type of housing and area; income source such as part-time or full-time employment, pension, reliance on savings, etc. This helps the men’s shed understand the client’s circumstances.
What high priority physical, emotional or social challenges is this person facing? Please try to describe them in as much detail as necessary.
What are the economic implications of these challenges?
What solutions does this person envision that will assist her or him to resolve or mitigate the challenge?
Many proposed solutions will involve the integration of smart house or internet of things technology into a residence or workplace. If so, it may be appropriate to solicit additional information. It has been my experience that many solutions are device dependent. At the same time clients are unable to use new or different devices or technologies. This is why in question 1, such specific information is requested.
What devices is the client using? Phone – clamshell, smartphone; other personal devices – tablet, laptop, desktop; servers; input devices such as keyboards, mice and scanners; output devices, such as televisions, screens and printers; Everything else that is hooked up to the internet with a cable, or without. If you have any idea about make and models and features, that would be helpful, as would any prices actually paid – new or used.
What is this person using these devices for? This is an important question, and arbitrary limits should not be put on it.
What communications and related services are being purchased/ provided? How are they being delivered? What do they cost? For example, some people have a landline incurring a monthly charge; some people are visiting coffee shops to use wifi connections; some people have cable television and/ or broadband and/ or dial-up internet and/ or alarm systems and/ or ???
What would this person want to use devices for, if a device had the necessary attributes, and service providers made services available either free, or at an affordable price? The essence of this question is, what does this person really want from his or her devices?
Men are human. This simple, three word sentence may come as a surprise to many, be they male or female. Women affected by #MeToo! misuse, may find it difficult to accept that men can be anything but low-life. Members of another gender may regard themselves as Übermenschen, supermen.
Some members of this male half of humanity, can be confused by the mixed signals they receive. On the one hand, they should suppress emotion and be strong, independent, stoic and tough. On the other, they should express their feelings openly and work co-operatively.
Admittedly, the stronger sex may also receive mixed signals, and sometimes they even give them – I’m told. However, this weblog post is (mostly) about the weaker sex, men.
Shoulder To Shoulder = slogan, shortened from: Men don’t talk face to face, they talk shoulder to shoulder.
Shedder = user of a men’s shed
Shedagogy = term coined by Barry Golding in 2014, to describe a distinctive, new way of acknowledging, describing and addressing the way some men prefer to learn informally in shed-like spaces mainly with other men.
In referencing this report it was difficult to know what to quote, mention or dismiss. It is ten years old and Australia specific, but includes nuggets of insight that have application elsewhere. Compared with women, men live shorter lives, have worse health, suffer 70% of injuries, commit 75% of suicides, access health services less and delay seeking health services more, spend less time with doctors, focus on physical problems, avoid discussing mental and emotional problems and ….
These facts are mixed with myths. Men are to blame for the world’s evils, including their own poor health and health outcomes. Men control social, occupational, political, environmental and economic environments. Men experience health services as a service for women and children. Men are socially conditioned to engage in risky behaviours from an early age
Sheds are important in male culture. Traditionally, sheds are spaces where men have retreated from work, life and family to make or repair things and to enjoy the company of other men. Unfortunately, the backyard shed is on the decline. Combined with other factors, such as retirement or loss of a partner, this results in loss of social networks, self-esteem, sense of purpose and identity, and can cause adverse social and emotional health and well-being issues for many men.
Sheds have in common that they are spaces for men, but may be diverse in organisation, structure and function. They can offer socialisation (friendship, camaraderie), self-esteem and purposeful activity for a large cross-section of men: young men, unemployed men, older men, retired men, men with mental health problems, disengaged men, indigenous men and immigrant men.
In Australian, where the men’s sheds movement is most highly developed, it is still an under-acknowledged, under-resourced, grassroots movement, that remains (mostly) unintegrated with any form of health system. They emerged despite an absence of any policy framework, government support or co-ordination.
Misan writes, “…key criteria for success of men’s sheds include: ensuring local support; learning from others, including affiliation with a men’s shed support organisation from the outset; having multiple partners and supporters; a suitable location; secure funding; a skilled manager and management group; a good business plan together with a sound marketing, recruitment, and communication strategy; a wide range of activities for men to take part in; extended opening hours; and links with a larger organisation, including a health service that can provide support for health programs. Ensuring documentation and evaluation of outcomes is also helpful to demonstrating benefit and increasing the likelihood of attracting future funding.” (p. 13)
While every men’s shed is unique, they can be lumped into four categories: work, clinical, educational and recreational.
For those who want to remain active, work sheds focus on repair, restoration and construction. At the same time much of the work is directed to helping the local community. Clinical focused sheds help the local male community interact and discuss their health/ wellbeing issues. Educational sheds focus on improving skills and life qualities, often around a specific skill, such as cooking. Recreational men’s sheds promote more social activity in the local area
Virtual sheds also exist, and provide an online capability where members from all men’s sheds or living in more remote communities can actively communicate and be involved in numerous research, writing and photographic activities. For example, The International Historians Association has created a community shed for veteran responders which include police officers, firefighters, paramedics, rescue workers and the military who have injuries, in-capacities or disfigurements that make them immobile or unwilling to join local work sheds.
The roots of The Men’s Sheds movement go back to the 1980s in Broken Hill, New South Wales, Australia and the former miners. There is also mention of the Albury Manual Activities Centre, also known as “Albury Men’s Shed” which opened in 1978. The focus in Adelaide, South Australia was on gender-biased and inappropriate care of older men living with dementia in care settings, as well as with Ausralia’s Vietnam War Veterans.
Mensheds Australia was established as an institution in 2002, by Peter Sergeant and Ron Fox as an outcome of their Economic Gardening activities.
An increasing number of Men’s Shed are being started. While the movement began in Australia in (>900 locations) and quickly moved on to New Zealand (>50). In Europe there are shed organizations in England, Finland, Greece, Ireland (>200 sheds), Scotland, Sweden (Malmö) and Wales.
In USA there are sheds in Hawaii (3), Michigan (1), Minnesota (5), Ohio (1) and Wisconsin (2). See: http://usmenssheds.org/
In Canada they are found in Alberta (2), British Columbia (7), Manitoba (2), Ontario (3) and Quebec (2). See: http://menssheds.ca
It is the fondest hope that the makerspace now being constructed in Straumen, will become a part-time Men’s Shed. On the other hand, it is also hoped that this space will offer time and space to many divergent groups of people: young and old, male and female, immigrant and native, experienced and inexperienced, practical and theoretical.
The Shed in Malmö will be given the opportunity to end this post with a description of themselves: Shed i Malmö is a space where people come together to do stuff, but more importantly, socialise. It’s like a hobby room, only bigger and better equiped. It’s like a lounge room, only more durable. It’s like a social club, but with more activities than just cards. Sometimes life isn’t always positive or even a continuation of the past. There is a new message now, 2019 is going to be a year of rediscovery for Shed i Malmö: we’ve had to move out of our location and we’re still assessing our options. We are currently ‘closed for business’. Sorry. http://shedimalmo.se/
In a few weeks the festive season will be upon us: this conjoined event stretches from Christmas to New Year’s day, or – for some – Hanukkah, which starts and ends even earlier, from sunset, 2018-12-02 to nightfall, 2018-12-10.
Thomas Nast, 1881 Merry Old Santa Claus, the iconic image of Santa Claus
The social costs of this festive season are extraordinarily high. There is a peak in drug offenses, drunk driving and other forms of anti-social behavior. Traffic accidents increase, not just because of increased drug and alcohol consumption, but because people are driving tired.
Another challenge with Christmas is that people attempt to buy happiness, through expensive gifts. These do not make people feel any better, but can put people into debt.
Overeating is another factor that has a negative impact on health. While in many countries suicide rates are at their lowest in December, mental health issues peak. Once Christmas is over, there is a sharp rise in suicides, often peaking on New Year’s day. Excessive eating and drinking combined with inadequate exercise erodes physical and mental health, including but not restricted to insomnia, depression and stress.
If that is not enough, then the Christmas season signals a time to file for divorce, or in other ways end relationships, including friendships.
Perhaps the best introduction to an American Christmas is Penne Restad’s Christmas in America. (Oxford University Press, 1995).
The celebration of Christmas is not an old tradition. It was not even a holiday until the middle of the 19th century. In the United States, the American Civil War combined with urbanization and industrialization helped to promote it as a means of creating social unity. Prior to this, people of different denominations followed traditions brought with them from Europe. With improved communication and transportation, there was a greater awareness of ethnic and religious pluralism. At the same time, there was increased political and economic tension between regions, and groups. Soon Darwinism and science were challenging religion.
This 19th century Christmas gradually transformed itself into a family gathering that merged faith with commercialism. Yes, people may attend church services, but it was not the church, but the house that was the focal point of the holiday.
Christmas trees were in use by 1832. By the 1850s, Christmas was fully entrenched in Northern cities. After the Civil War, it captured the South.
Christmas tree ornaments emerged about 1870, with imports from Germany. While there were some Christmas cards in the early 1850s, demand exploded by about 1875. These soon replaced the more traditional Christmas letter.
Christmas gift-giving had its origins in the 1870s. Part of this was related to problems of extreme economic inequality that threatened social relationships. Thus, many of the gifts were charitable.
The American Christmas is incomplete without Clement Moore’s An Account of a Visit from Saint Nicholas in the 1820s. Here is the spirit of Christmas in the persona of Santa Claus, with fur-trimmed red suit, sack of toys, reindeer, sleigh and home at the North Pole.
Christmas dinner is so notable that it warrants its own Wikipedia article. See: https://en.wikipedia.org/wiki/Christmas_dinner
So how should Christmas be managed to avoid its negative aspects? The answer is to build more work-like attributes into it.
Activities should be planned, and scheduled. People should know what is happening, and what they personally are expected to do.
In the build-up to Christmas, people can be asked to design Christmas cards, to write an annual Christmas letter and/ or to plan meal menus. They should also use their skills to design and make decorations and presents. To reduce costs, guidelines can be given that make these more appropriate. For example, gifts are to be made from re-purposed materials.
Alcohol is not part of a normal work week, and (for me) there is no reason why it should be part of a leisure event, such as Christmas. Avoiding alcohol is yet another way to reduce costs, and to ensure relationships endure. To prevent meals from expanding waistlines, there should be calorie limits in place, and moderate quantities. At Cliff Cottage, the permanent residents weigh themselves daily. Some people make their weight publicly available, while others keep it private.
When families get together to celebrate, there should be fixed times to arise, and to head off to sleep. There should be opportunities for exercise, and opportunities for every individual to be alone. Child-minding should be an activity distributed among the adults.
While there may be a desire to spend some time listening to music, or watching a film, moderation is also a key here. In fact, it could be more fun to sing, or perform musically together, rather than to listen to someone else’s efforts. Perhaps, the entire family could have fun making a video, rather than watching someone else’s.
Let us all make Christmas fun again, but putting structure and moderation in place during Christmas, 2018!